Protein Density: The Metric That Matters on GLP-1
You're eating less on GLP-1 medication. That's the entire point. Semaglutide and tirzepatide suppress appetite, slow gastric emptying, and make large meals physically uncomfortable. Fewer calories in, weight goes down.
But here's the part that doesn't make it into the marketing: up to 40% of weight lost on GLP-1 medications can be lean body mass. Not fat. Muscle, bone density, the metabolic engine that keeps you healthy long after the prescription ends.
The metric that determines which side of that split you land on isn't total protein. It's protein density.
The lean mass problem
GLP-1 receptor agonists work. They reduce appetite dramatically. People who used to eat 2,000-2,200 calories find themselves comfortable at 1,200-1,400. That's a 40% reduction in total food intake.
The math gets brutal fast. If someone was eating 170g of protein across 2,000 calories and drops to 1,300 with the same food choices, they're getting roughly 110g. That's a 35% cut in the raw material their body needs to maintain muscle.
Standard protein targets (the "eat X grams per day" kind) become nearly impossible at suppressed calorie levels. You can't hit 170g on 1,300 calories eating the same foods you ate at 2,000. Those foods had too many accompanying calories from carbs and fat.
This isn't a willpower problem. It's a density problem.
What is protein density?
Protein density is grams of protein per 100 calories of food. It strips away portion size and total calories and asks one clean question: how much muscle-preserving protein does each calorie deliver?
The tiers:
| Density Tier | Grams per 100 kcal | What It Means | |---|---|---| | Excellent | 8g or more | Maximum muscle preservation per calorie | | Good | 5-8g | Solid contribution without wasting caloric budget | | Adequate | 3-5g | Acceptable, but not moving the needle | | Low | Under 3g | Mostly fueling everything except muscle |
What this looks like with real food:
- Chicken breast: ~13g per 100 kcal. Almost pure protein delivery.
- Greek yogurt (plain, nonfat): ~10g per 100 kcal. One of the best density-to-convenience ratios out there.
- Eggs: ~8g per 100 kcal. Right at the excellent threshold. Fat content costs some density.
- Salmon: ~7g per 100 kcal. Good. The omega-3s make the tradeoff worth it.
- Almonds: ~4g per 100 kcal. Adequate. Most of the caloric load is fat.
- Rice: ~2g per 100 kcal. Low. It's an energy source, not a protein source.
A handful of almonds feels protein-rich. And at 6g per serving, it's not nothing. But when you only have 1,300 calories to work with, those 160 calories delivered just 4g per 100 kcal. The same calories from chicken breast would deliver over three times the protein.
Why density beats volume on GLP-1
When your appetite is suppressed and your stomach empties slowly, every bite carries disproportionate weight. There is no "eat more" option.
Consider two lunches:
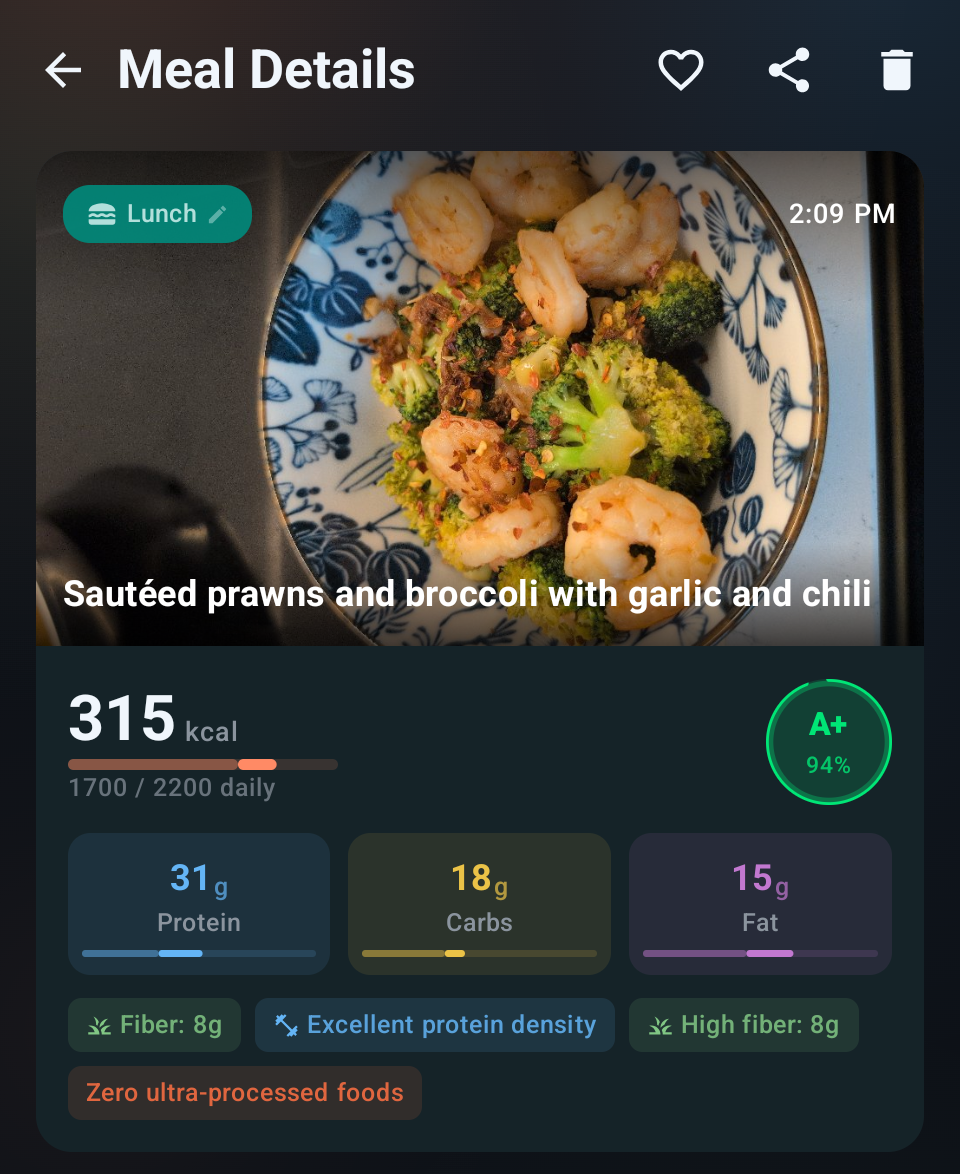
Lunch A: Grilled chicken over greens with lemon vinaigrette. 300 calories, 35g protein. Density: 11.7g per 100 kcal.
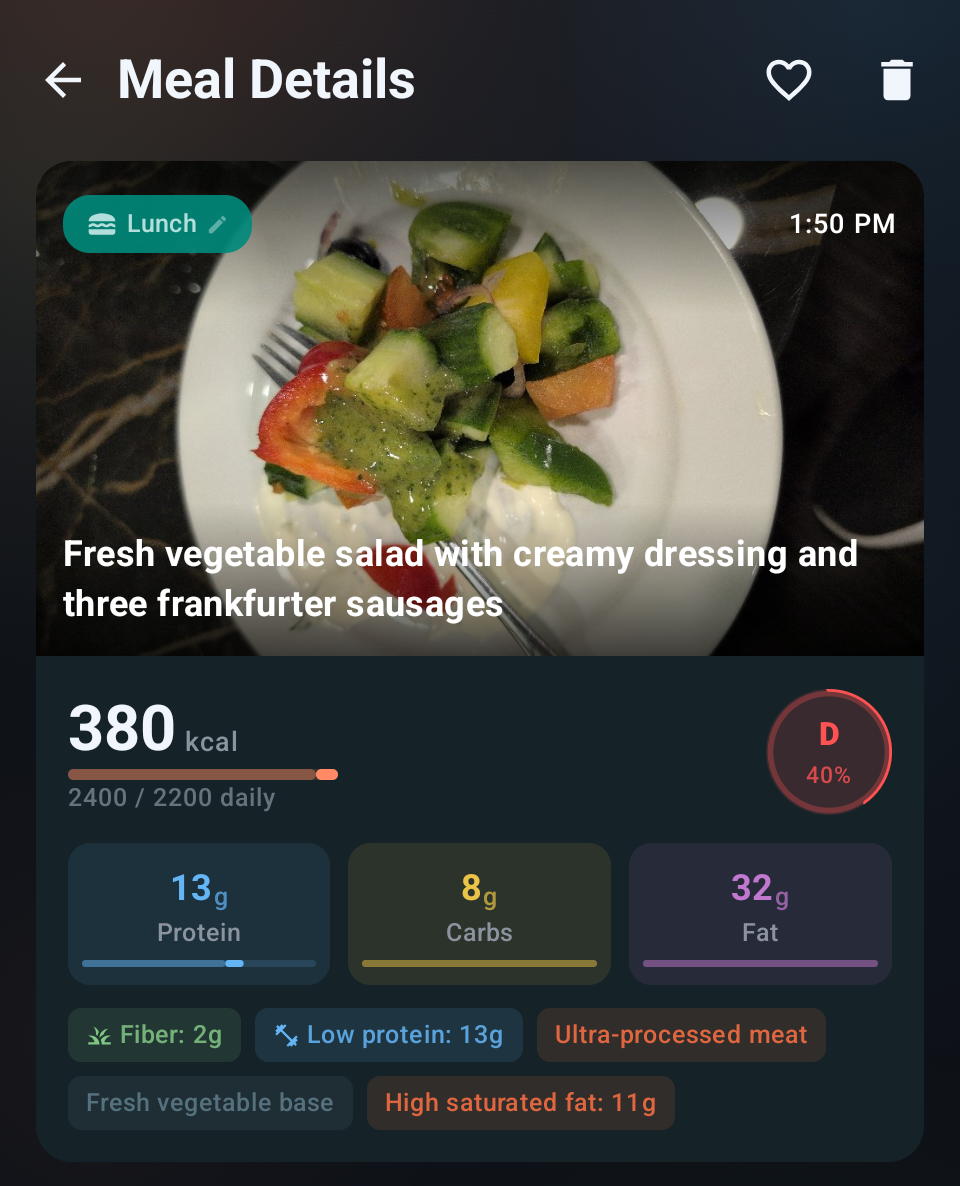
Lunch B: Turkey sandwich on sourdough with avocado and cheese. 600 calories, 32g protein. Density: 5.3g per 100 kcal.
Lunch A delivers more protein in half the calories. For someone on GLP-1 medication who physically can't finish a large meal, this is the difference between preserving muscle and slowly losing it. The sandwich isn't bad food. It's just a poor use of limited caloric real estate.
This is the shift in thinking GLP-1 users need. The question changes from "does this meal have enough protein?" to "does this meal have enough protein for the calories it costs?"
At 2,000 calories a day, you can afford some low-density meals and make up the difference elsewhere. At 1,300, there is no elsewhere.
How MyProtocol uses this
I built MyProtocol with this problem in mind. GLP-1 mode treats protein density as the primary scoring signal.
Scoring adapts to your reality. Meals are evaluated on composition, not calorie volume. A 200-calorie meal with 25g of protein (12.5g per 100 kcal) scores as exceptional. The small portion isn't a problem. It's expected.
The coach never tells you to eat more. Reduced appetite is a feature of your medication, not a bug. Suggesting "just eat another meal" is tone-deaf guidance that ignores why you're on GLP-1 in the first place. Instead, the feedback focuses on swaps: same meal, denser protein choices.
Exceptional density gets recognized. Hit above 12g per 100 kcal and the feedback reflects it. Not generic praise, but specific acknowledgment that you're protecting lean mass effectively.
Building a density-first plate
The practical application is simple. Before each meal, rank your options by density:
Start with your protein source. Chicken, fish, egg whites, shrimp, Greek yogurt, cottage cheese. All above 8g per 100 kcal. They form the foundation.
Add vegetables freely. Most are so low in calories they barely register, while adding fiber, micronutrients, and satiety.
Be strategic with fats. Fats are 9 calories per gram, more than double protein and carbs. A tablespoon of olive oil adds 120 calories with zero protein. That doesn't make olive oil bad. It means you account for it rather than pour freely.
Audit your carb sources. If rice is taking up 300 of your 1,300 calories and contributing 6g of protein, ask whether that caloric space could work harder. Sometimes the answer is still rice. But make it a conscious choice.
The goal isn't perfection on every plate. It's awareness of where your protein is actually coming from, and whether the calories around it are earning their place.
The bottom line
GLP-1 medications changed the weight loss landscape. But the conversation hasn't caught up to the nutritional reality they create. Eating less is only half the equation. Eating dense is what determines whether the weight you lose is the weight you want to lose.
Protein density is the single most useful metric for anyone on appetite-suppressing medication. It cuts through portion anxiety, simplifies food choices, and directly correlates with lean mass preservation.
Not sure what your daily target should be in the first place? The free GLP-1 protein calculator gives you a number and a per-meal breakdown in ten seconds.
Your appetite is smaller now. Make every calorie count.
Like our approach?
MyProtocol scores your meals, coaches you in real time, and adapts to your goals. Get started in two minutes.